
An ACPE application based activity
In 2006, the World Health Organization (WHO) began the High 5s programme. Medicines reconciliation was a target and due to the complexity and resource requirement, their focus was on patients 65 years of age and older, who were admitted to an inpatient ward from the emergency department. The Institute of Healthcare Improvement (IHI) also set medicines reconciliation as one of its work streams in their ‘Saving Lives campaign’. In the UK from 2004 to 2008, IHI together with the Health Foundation (HF) launched the Safer Patients Initiative. They also set a target on medicines reconciliation and acknowledged that this could be a slow process due to the complexity.
Medication Reconciliation is defined by the US Joint Commission as “the process of comparing the medications a patient is taking (and should be taking) with newly ordered medications”. It is designed to ensure that a patient’s medication history is identified and addressed in the hospitalization process. When organisations do not consistently and reliably reconcile patient medications across the continuum of care, medication errors and adverse drug events occur. About 20% of all adverse drug events have been attributed to poor communication at the transition and interfaces of care.
Medicines reconciliation has been an emerging topic in EAHP Congresses for a couple of years. Although there is no objection to the importance, no uniformity could be seen in the methodologies used in submitted abstracts. This lacking part of quality management and pharmaceutical support is one of the declared targets to explore in this Academy seminar. The topic is too important to let grow a multitude of not harmonised methods and develop an auto-dynamic reconciliation practice in European hospitals.
Evidence is needed to demonstrate that pharmacists do best medicines reconciliations. The reality of the staffing situation must be evaluated, if hospital pharmacy should warrant an added value of its performance and capabilities, performances by technicians and nurses, while being supervised by a pharmacist, must be assessed. There must be clarity in the responsibility for the SOPs, training and the more complex medicines reconciliations. For all those who are new in medicines reconciliation, practicalities should be harmonised all over Europe: How to set up the service? How to staff? When to do medicines reconciliation (only on admission if resources are short?)? How to get the necessary logistics changes done in the hospital medication list? How to document medicines reconciliation in the case notes? What "added extras" can medicines reconciliation offer?
Lots of interfaces to other disciplines are needed to effectively and successfully reconcile medications. Pharmacy contribution to multidisciplinary task forces is likely to have added values, according to studies, which focus mainly on patient admission. This should be expanded as a continuing reconciliation and support until the patient's discharge, thus from Medicines Reconciliation to Medicines Optimisation and Medicines Review.
Reconciliation is at the interface of procurement, clinical pharmacy and patient safety. It is also addressed in the European Statements of Hospital Pharmacy. According to statement 2.7, hospital pharmacists should be involved in the development of policies regarding the use of medicines brought into the hospital by patients. In addition, according to statement 4.4, all the medicines used by patients should be entered on the patient’s medical record and reconciled by the hospital pharmacist on admission. Hospital pharmacists should assess the appropriateness of all patients’ medicines, including herbal and dietary supplements. In line with statement 5.6, hospital pharmacists should ensure that high-risk medicines are identified and implement appropriate procedures in procurement, prescribing, preparing, dispensing, administration and monitoring processes to minimise risk. As a result, the hospital pharmacy contribution to medications reconciliation consists of:
In addition to these European Statements of Hospital Pharmacy, the need is also arising from hospital pharmacy practice, since the topic "medication reconciliation" has been proposed in the Cyber Café Survey at the EAHP Congress 2014 in Barcelona and from the EAHP Scientific Committee.
The needs, the contents and the findings of this Academy seminar will cover the following statements of the European Statements on Hospital Pharmacy:
Teaching goals:
The target group comprises clinically oriented hospital pharmacists at the interface of R&D and practice, mainly heads and/or deputy heads of pharmacy, particularly those from the new EU countries and new members of EAHP.
There will be introductory lectures about the most relevant subchapters of medicines reconciliation right before the workshops will start. The messages delivered during the introductory lectures will be applied and systematised in breakout sessions and plenary discussions. Breakout sessions will serve to develop a catalogue and classification, statements, standards and policy drafts, checklists and guidelines or recommendations. Communication methods used in medicines reconciliation will be demonstrated as well as trained and peer-reviewed in plenary. Groups are selected according to country-similarity. Flow-charts and mind maps will be designed using X-mind® freely available on the web. Laptops, beamers (and flipcharts), handycam / video equipment will be used as didactic and e-learning tools.
The EAHP has partially delegated evaluations of the Academy Camps to the National Associations. In general, presentations and workshop results will be reported back to the associations' members as presentations in the course of General Assemblies or at separate symposia. To facilitate reporting and multiplying knowledge in the national associations, delegates will receive summary slides from the presentations and documents from the workshops. National Assemblies confirm the completion of multiplication to EAHP.
Dr Fatma Karapinar, Epidemiologist, Sint Lucas Andreas Ziekenhuis, Amsterdam, the Netherlands
Abstract
In daily practice, medication reconciliation is too often seen as a process to obtain a medication list without an evaluation regarding what's on the list. It involves a three-step process:
In daily practice generally only the verification step is performed. Any new medication added is not evaluated. Therefore, there are still patients who are discharged with hypnotics, laxatives, proton pump inhibitors etc. which do not have an indication anymore at discharge. Medication reconciliation at hospital discharge focuses too often on admission, but the length of stay decreases in hospitals. For continuity of pharmaceutical care, thus the focus needs to be aimed at discharge and on collaboration with primary care as well. The process at discharge is far more complex that it is at admission. The consequences can also be major (e.g. a physician that forgets to re-start anticoagulation after a surgery). Also there are multiple problems post-discharge. A recent study showed that patients have DRPs within 72 hours post-discharge, despite medication reconciliation at hospital discharge. So hospital pharmacists need to think broader than the walls of their hospitals.
Further challenges of medication reconciliation comprise:
Teaching goals
In this section, the presenter will:
Learning objectives
At the end of this session, participants will be able:
Mrs Jane Smith, Principal pharmacist, Development & Governance, NBT Medication Safety Officer (MSO), North Bristol NHS Trust, Bristol, UK
Abstract
"The aim of medicines reconciliation on hospital admission is to ensure that medicines prescribed on admission correspond to those that the patient was taking before admission. Establishing correct medications details may involve discussion with the patient and/or carers and the use of records from primary care. "
In some countries this process also includes a review of the Patients Own Drugs (PODs). Medicines Reconciliation should occur on admission, on transfer and on discharge. This workshop will focus on medicines reconciliation on admission because this is a complex area as information from primary care and patients and/or carers is not always easy to obtain. Furthermore, patients do not always use their medicines the way their health professionals think.
Our experiences of achieving medicines reconciliation have involved the use of quality improvement tools (for example the "Safer Patients Initiative" involving the use of the Model for Improvement and PDSA (plan, do study, act) cycles). Typically, this can begin on one ward, followed by ongoing tests of change, measurement and displaying run charts to spread and embed medicines reconciliation.
Pharmacists and Pharmacy Technicians, thanks to their expertise and training, have an opportunity to help lower the burden of medication discrepancies through their input in Medicines Reconciliation.
Teaching goals
In this section, the presenter will:
Learning objectives
At the end of this session, participants will be able:
Dr André Rieutord, Hôpital Antoine Béclère/ Service Pharmacie, Clamart, France
Abstract
The pharmacy of Antoine Béclère Hospital experienced 6 years of practice in different clinical settings. We consider that starting Medication reconciliation is very exciting but one always has to consider the sustainability of the process when implemented. Through our medication reconciliation story board, we will highlight problems encountered after implementation. The pharmacist as any project manager must define a strategy, identify the barriers (human factors, quality, training, technology...) and propose collaborative solutions according to the given context. Business process improvement using "Kaizen" approach will be considered and illustrated with concrete examples.
Teaching goals
In this section, the presenter will
Learning objectives
At the end of this session, participants will be able:
Prof Dr Tommy Eriksson, Lund University, Lund, Sweden
Abstract
The Lund Integrated Medicines Management (LIMM) -model with pharmacists as the driver has been developed, researched and implemented over 15 years. Now the model has been fully implemented in the eight hospitals of the County of Skåne (south of Sweden). The Med Rec process is the base for the team activities where the pharmacist and the physician has different but complementary roles. Clinical-, economic- and humanistic outcomes will be presented based on patient focus and safety, quality, systematic activities, educational aspects and payment for performance. There will also be a focus on discharge Med Rec. What information do the patient and the next level of care need and how can it be presented and communicated.
Teaching goals
In this section, the presenter will:
Learning objectives
At the end of this session, participants will be able:
Dr Ulrika Gillespie, Uppsala University Hospital, Uppsala, Sweden
Abstract
Many studies have been performed worldwide to try to determine the magnitude and consequences of medication errors that occur when patients are being transferred between caregivers. Again, many studies have looked into the effects of different strategies aiming at minimizing the risk of errors. In this session the focus is on the effects of medication reconciliation performed by pharmacists and on trying to summarize the current evidence base.
Medication reconciliation is sometimes carried out without including a patient interview (mostly due to time constraints). There is debate however, to whether it is even possible to claim that a medication reconciliation has been performed if the patient has not been involved, confirming the actual use of the drugs on the reconciled list. In this session the importance of the additional information gained from the interview will be demonstrated and discussed along with a description of key items to include in the interview.
Teaching goals
In this section, the presenter and workshop coach will
Learning objectives
At the end of this session, participants will be able
Prof Dr Tommy Eriksson, Lund University, Malmö, Sweden
Dr Ulrika Gillespie, Division of Pharmacokinetics and Drug Therapy, Department of Pharmaceutical Biosciences, Uppsala University and Uppsala University Hospital, Uppsala, Sweden
Abstract
The oral structured clinical examination by the hospital pharmacist comprises the two steps as follows:
Teaching goals
In this section, the presenter sand workshop coaches will:
Learning objectives
At the end of this session, participants will be able:
Abstract
The afternoon presentations and the afternoon workshop will consist of a demonstration of the structured interview technique followed by the integration of the delegates into a discussion and evaluation of the demo interviewing, as well as role plays after the coffee break. In order to train typical communication scenarios between pharmacist and patient, role plays of the structured patient interview will give the delegates a representative impression of best practice and of using standardised procedures to train pharmacists in medication reconciliation. The role plays will be registered and video sequences discussed in plenum.
Teaching goals
In this section, the workshop coaches will:
Learning objectives
At the end of this session, participants will be able:
Abstract
In order to evaluate added values for the therapist (and their interest in the clinical outcome), for taxpayers (and their interest in the financial outcome), and for patients (and their interest in extended QALYs), an interactive podium discussion on further elements and the interfaces at patient admission and discharge is held. Current approaches of medicines reconciliation concentrate on admission and on discharge. Supervision of further aspects of pharmacotherapy along the entire hospital stay may contribute to better outcomes as well. The pharmacist's contribution to medicines reconciliation, optimisation and review may comprise laboratory data (point of care testing), or the phenotype of the patient.
The interactive podium discussion will be a moderated discussion and will include presumably items such as "the Gold Standard - pharmacy and/or patient's records", qualification aspects, training aspects, inappropriate pharmacotherapy, "beyond simple lists - drug related problems to be reconciled".
Elements of this discussion will be used in the following parallel workshop on systematisation.
Teaching goals
In this section, the workshop coaches will:
Learning objectives
At the end of this session, participants will be able:
Abstract
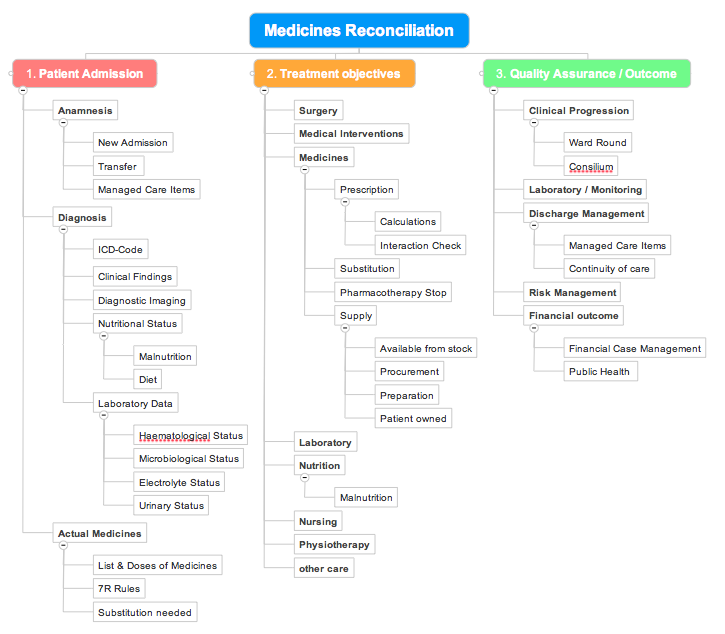
Inputs from the introductory presentations arising from research and practice now have to be recombined to a comprehensive overview of the relevant elements of medicines reconciliation. Experiences of the delegates and regional or national approaches have to be brought together. The catalogue of the elements of medicines reconciliation will be broken down into a consistent workflow of single steps, which starts at the anamnesis and ends with the complete medication log in the electronic patient documentation at discharge.
The 4 parallel workshops will develop the following take home deliverables:
- Medicines Reconciliation on Admission
- Integrated Medicines Management on the entire hospital stay
- Medicines Reconciliation on Discharge
Teaching goals
In this section, the workshop coaches will:
Learning objectives
At the end of the workshops, participants will be able:
References
Links
[1] http://www.nice.org.uk/guidance/psg001/evidence/full-guidance-pdf2
[2] http://www.jointcommission.org
[3] http://www.hospitalpharmacyeurope.com/featured-articles/improving-medicines-reconciliation-admission
[4] http://gruposdetrabajo.sefh.es/genesis/index.php?option=com_content&view=article&id=13&Itemid=15